India set to launch free nationwide HPV vaccination for adolescent girls
Table of Contents
Relevance: GS Paper II – Health / Social Sector (Govt policies & interventions, public health)
GS Paper III – S&T / Biotechnology (vaccines, disease prevention, health tech platforms)
For Prelims:
- HPV (Human Papillomavirus), Cervical cancer, Gardasil (quadrivalent), HPV 16 & 18 (high-risk), HPV 6 & 11 (low-risk), Single-dose schedule, Voluntary & free vaccination, Gavi Vaccine Alliance, CDSCO, NTAGI, Cold chain, AEFI (Adverse Events Following Immunisation), Ayushman Arogya Mandir, U-WIN platform, Pap smear, HPV DNA test, WHO 90–70–90 targets.
For Mains:
- Cervical cancer elimination strategy, Preventive healthcare, Vaccine equity, Adolescent health, Screening + vaccination integration, Behavioural/biomedical/structural interventions, Health system preparedness, Digital health governance (U-WIN), Public communication & vaccine hesitancy, Global health partnerships (Gavi), SDG 3.3, Women’s health burden reduction.
Why in News?
- Union Health Ministry is set to launch a nationwide HPV vaccination programme for girls aged 14 years.
- Vaccination will be voluntary and free of cost, to ensure equitable access across socio-economic groups.
- India will use Gardasil (quadrivalent HPV vaccine) and is adopting a single-dose regimen (with an optional delayed second dose after 3–5 years, as per the notes you shared).
- The programme is grounded in NTAGI recommendations, national disease burden evidence, and global best practices.
Background
- Cervical cancer is largely preventable through HPV vaccination + early screening, yet continues to impose a heavy burden on women and families.
- India aims to align with global commitments to eliminate cervical cancer as a public health problem.
Key Facts of the HPV Vaccination Drive (India)
1) Target group & coverage
- Target: Girls aged 14 years (chosen because preventive benefit is highest before potential exposure).
- Nature: Voluntary + free nationwide programme.
2) Vaccine used
- Gardasil (quadrivalent) protects against:
- HPV 16 & 18 → major cause of cervical cancer
- HPV 6 & 11 → associated with genital warts/low-risk disease
3) Regimen and evidence
- Single-dose: “Global and Indian scientific evidence” indicates robust and durable protection when given at recommended age.
- Vaccine is non-live → does not cause HPV infection.
- Safety record: supported by 500 million+ doses globally since 2006.
- Effectiveness: evidence of 93–100% effectiveness against cervical cancer caused by vaccine-covered HPV types.
4) Procurement & quality assurance
- India secured supplies through a transparent, globally supported procurement mechanism.
- Under partnership with Gavi, the Vaccine Alliance, Gardasil (approved by India’s drug regulator) is being procured with stringent quality + cold chain standards.
- Note you provided: Cervavac (indigenous vaccine) is not yet WHO-approved for the programme.

Implementation & Safety
Vaccination sites (only govt facilities)
- Ayushman Arogya Mandirs (PHCs)
- Community Health Centres (CHCs)
- Sub-District & District Hospitals
- Government Medical Colleges
Safety protocols
- Sessions conducted in presence of trained medical officers + skilled teams
- Post-vaccination observation and readiness to manage rare adverse events
- All sites linked to 24×7 government health facilities for immediate support
- Programme style note you provided: conducted as a special campaign on designated immunisation days, not routine UIP, and tracked through U-WIN for rapid coverage.
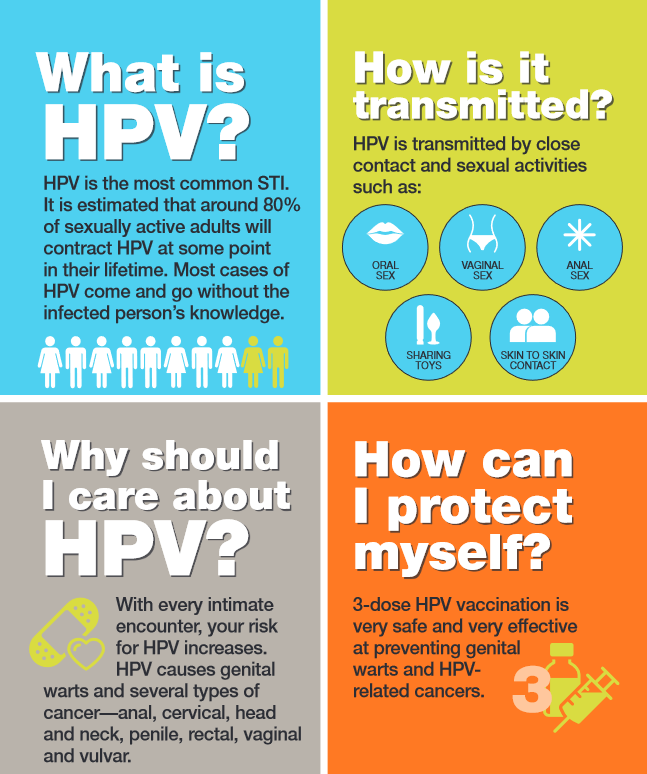
HPV Basics
- HPV: non-enveloped, double-stranded DNA viruses (Papillomaviridae), infect epithelial cells.
- Most infections are asymptomatic; about 90% clear within 1–2 years via immune response.
- High-risk (oncogenic): HPV 16, 18 → cancers
- Low-risk: HPV 6, 11 → warts
- Transmission: mainly intimate skin-to-skin contact, commonly sexual activity.
- Prevention toolkit (besides vaccine): condom use, voluntary male circumcision, smoking cessation, safe sexual practices.
Cervical Cancer Burden (India)
- 2nd most common cancer among women in India
- ~80,000 new cases and 42,000+ deaths annually
- Persistent high-risk HPV infection causes nearly all cervical cancers; in India, HPV 16 & 18 account for >80% of cases (as per your input).

HPV Vaccine is NOT a “Free Pass”
- Vaccine protects against common high-risk strains, but not all cancer-causing HPV types.
- Therefore, screening must continue:
- Pap smear (cytology) detects early abnormal cell changes
- Recommended screening begins at 21 years; and after 30, Pap + HPV DNA testing may be combined as per medical guidance.
- Vaccination after sexual debut still benefits, but cannot clear existing infections → screening becomes even more important.
Global Context
- 90+ countries are implementing single-dose HPV schedules to improve coverage and affordability.
- Several countries show reductions in HPV infection, pre-cancerous lesions, and cervical cancer incidence after widespread vaccination.
- WHO cervical cancer elimination targets (WHA 73.2) by 2030:
- 90% girls vaccinated by age 15
- 70% women screened (35 & 45 years)
- 90% treated if disease detected
- WHO response framework (2022–2030) also ties into broader STI control, and a 2021 WHO resolution on oral health includes measures addressing mouth/throat cancers (as per your notes).
Significance
- Women’s health protection: prevents HPV infection before progression to cancer.
- Equity: free vaccination across all States/UTs reduces socio-economic gaps.
- Public health impact: potential major fall in cervical cancer burden over time.
- Systems strengthening: cold chain, trained staff, safety linkage to 24×7 facilities, and digital tracking (U-WIN) improve programme quality.
Challenges
- Awareness + myths (vaccine hesitancy; misunderstanding that screening is unnecessary)
- Ensuring high coverage in hard-to-reach areas
- Cold chain + session quality at scale
- Integrating vaccination with screening rollout, because screening uptake is low in India (as your provided background hints)
Way Forward
- Strong IEC campaign: “Vaccine + screening together”
- School/community mobilisation for adolescent coverage
- Strengthen screening services and referral pathways
- Use U-WIN for follow-up, AEFI reporting, and coverage gaps
- Continue evaluating indigenous options like Cervavac as approvals evolve
Conclusion
India’s free, voluntary national HPV vaccination programme for 14-year-old girls is a major preventive health step to reduce cervical cancer. Its success will depend on achieving high coverage, maintaining cold-chain and safety standards, and ensuring that vaccination is paired with sustained cervical cancer screening.
UPSC PYQ
Q. ‘Mission Indradhanush’ launched by the Government of India pertains to (2016)
(a) immunization of children and pregnant women
(b) construction of smart cities across the country
(c) India’s own search for the Earth-like planets in outer space
(d) New Educational Policy
Ans: (a)
CARE MCQ
Q. With reference to India’s HPV vaccination programme, consider the following statements:
- Gardasil used in the programme protects against HPV 16 and 18 as well as HPV 6 and 11.
- HPV vaccination eliminates the need for future cervical cancer screening.
- Vaccination will be provided only through designated government health facilities and monitored for rare adverse events.
Which of the statements given above is/are correct?
A. 1 and 3 only
B. 1 only
C. 2 and 3 only
D. 1, 2 and 3
Answer: A
Explanation
- Statement 1 – Correct: Gardasil is quadrivalent (16/18 + 6/11).
- Statement 2 – Incorrect: Vaccine does not replace screening; Pap smears/HPV tests still matter.
- Statement 3 – Correct: Govt facilities + trained staff + observation/AEFI preparedness + 24×7 linkage are part of the plan.